

Background: The rhesus (Rh) and Kell blood group systems are the most common of over 50 different antigens capable of causing maternal red blood cell (RBC) alloimmunization and severe fetal hemolytic disease. Anti-K and anti-D are responsible for a significant proportion of fetal anemia requiring intrauterine transfusion (IUT). Whilst IUT of packed RBCs improves neonatal survival and morbidity, clinical prognostic indicators are lacking. Our primary objective was to identify predictors of adverse outcome.
Methods: We conducted a retrospective single-center study at Mount Sinai Hospital (MSH), Toronto, Canada. All pregnant patients alloimmunized with anti-K and anti-D as a single antibody, between 1991 and 2018 were included. Data were obtained from patient medical records, ultrasound reports and information from the transfusion medicine laboratory. Data included maternal demographics, antibody titers, pregnancy history, number of IUTs, hemoglobin (HB) concentration at the beginning and end of all IUTs. Neonatal outcomes included survival, mode of delivery, gestational age at delivery, birth weight, HB at birth and need for neonatal transfusion, phototherapy or intravenous immunoglobulins (IVIG). Our primary outcome was the composite outcome of stillbirth or neonatal death (SB/NND). We also constructed a secondary outcome consisting of top-up neonatal transfusion, exchange transfusion, phototherapy, or use of IVIG. Medians and interquartile ranges (IQR) or mean±SD were used as summary statistics and compared by Mann-Whitney or t-test; p<0.05 was statistically significant. Outcome predictors were identified using multivariable logistic or linear regression analysis; accounting for patient level clustering by marginal Generalized Estimating Equation did not significantly affect variables. Data were analyzed using SPSS.
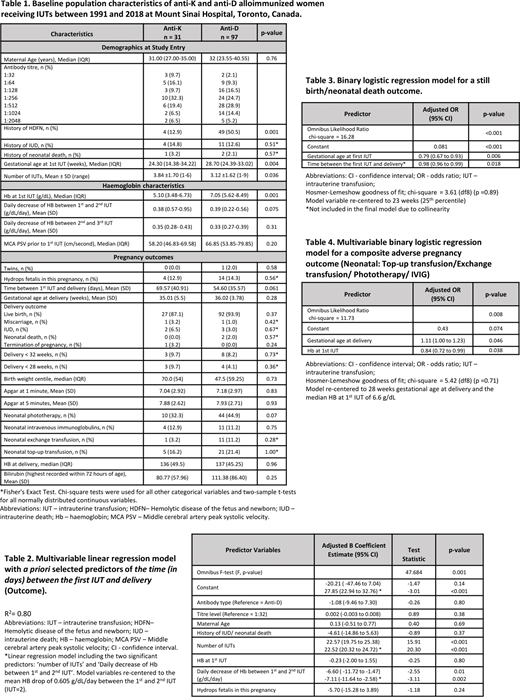
Results: 116 women with 128 pregnancies and 425 IUTs with anti-K or anti-D as a single antibody were identified. Median maternal age was 31 years (27.0-35.0) for anti-K and 32 years (23.6-40.6) for anti-D. The gestational age at 1st IUT differed significantly between anti-K and anti-D (24.3 vs 28.7 weeks respectively, p=0.004). Women with anti-K antibodies required more IUTs than women with anti-D (3.84 vs 3.12 IUTs, p=0.036) and HB at 1st IUT was significantly lower in the anti-K group (5.10 vs 7.05 g/dL, p=0.001) (Table 1). Following initiation of IUT, the time from 1st IUT to delivery was 69.6 days in the anti-K group and 54.6 in the anti-D group (p=0.06). The daily decrease of HB between 1st and 2nd IUT (as a marker of disease severity), development of fetal hydrops and severe preterm birth did not differ significantly between the two groups. Mean gestation age at delivery was 35.0 weeks in the anti-K and 36.0 weeks in the anti-D group (p=0.28), with 87.1% and 93.9% survival (p=0.37), respectively. The proportion of neonates requiring phototherapy, IVIG and exchange/top-up transfusion was comparable across the two antibody groups (Table 1).
Regression analysis showed that delivery occurred sooner if HB dropped more rapidly between the first two IUTs (p=0.01). Each additional transfusion gained on average 22.5 days in utero (Table 2). In multivariable analysis, gestational age at 1st IUT was the only predictor of a SB/NND outcome (adjusted OR 0.79 [95%CI 0.67-0.93]; p=0.006). With 1st IUT at 23 weeks, the risk of SB/NND was 8%, but only 2.5% at 28 weeks and <0.01% at 36 weeks (Table 3). Gestational age at delivery (adjusted OR 1.11 [95%CI 1.00 to 1.23]; p=0.046) and HB at 1st IUT (adjusted OR 0.84 [95%CI 0.72 to 0.99]; p=0.038) were the only predictors of a composite adverse blood product requirement/intervention outcome (Table 4). The odds of blood product requirement/intervention postnatally at 1st IUT (median HB at 1st IUT of 6.6g/dL) at 28 weeks were 43% and increased by a further 38% for delivery at 34 weeks.
Conclusion: The earlier in gestation that IUTs are implemented, the higher the odds of a SB/NND; however the later the gestation at delivery, the greater the odds of the neonate requiring blood products post-partum. The greater the HB drop between the 1st and 2nd IUT, the shorter the 'time between the first IUT and delivery', which increases the odds of a SB/NND outcome.
Garbowski:Vifor Pharma: Consultancy, Membership on an entity's Board of Directors or advisory committees; Imara: Consultancy. Shehata:Ferring: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal